The effect of sleep on blood biomarkers
When patients ask us “what does sleep actually change in my blood?”, the honest answer is that very few studies look at it directly. Most sleep research ties bad nights to disease outcomes (heart attacks, dementia, mortality), not to the panels your annual labs measure. So we ran the analysis ourselves.
We pulled 7,033 paired observations from Empirical Health members who track sleep on Apple Watch or other wearables and who have ordered a blood test. Each pair lined up a biomarker result with the average of at least 18 nights of sleep data leading up to the draw. Across 444 biomarker × sleep-metric pairings, 79 reached p<0.05 and 15 reached p<0.001. By chance alone we’d expect about 22 at p<0.05, so the data contains roughly 3.5x more real signal than noise.
The strongest signals show up where you’d hope: immune cell ratios, blood sugar, and the restorative-stage markers. The rest of this post walks through the highest correlations in the matrix and what they suggest about which sleep dimensions actually move the needle.
TL;DR: Sleep quality and duration each move a long list of blood biomarkers. The strongest, cleanest signals are in immune cell ratios and glucose.
How many sleep-vs-biomarker correlations are statistically significant?
We tested 74 biomarkers against six sleep dimensions: quality, duration, deep sleep %, REM sleep %, sleeping HRV, and night-to-night consistency. That’s 444 pairings. By chance alone, around 22 would clear p<0.05.
We found 79. Sleep quality (our composite that blends duration, stages, and physiology) led the pack with 24 significant correlations, followed by deep sleep % and duration tied at 17, REM sleep % at 11, night-to-night consistency at 7, and sleeping HRV at 3. The fact that quality dominates isn’t a tautology. Most blood markers don’t track any one sleep variable cleanly, so a composite score ends up doing more work than its parts.
Sleep quality and immune cell balance
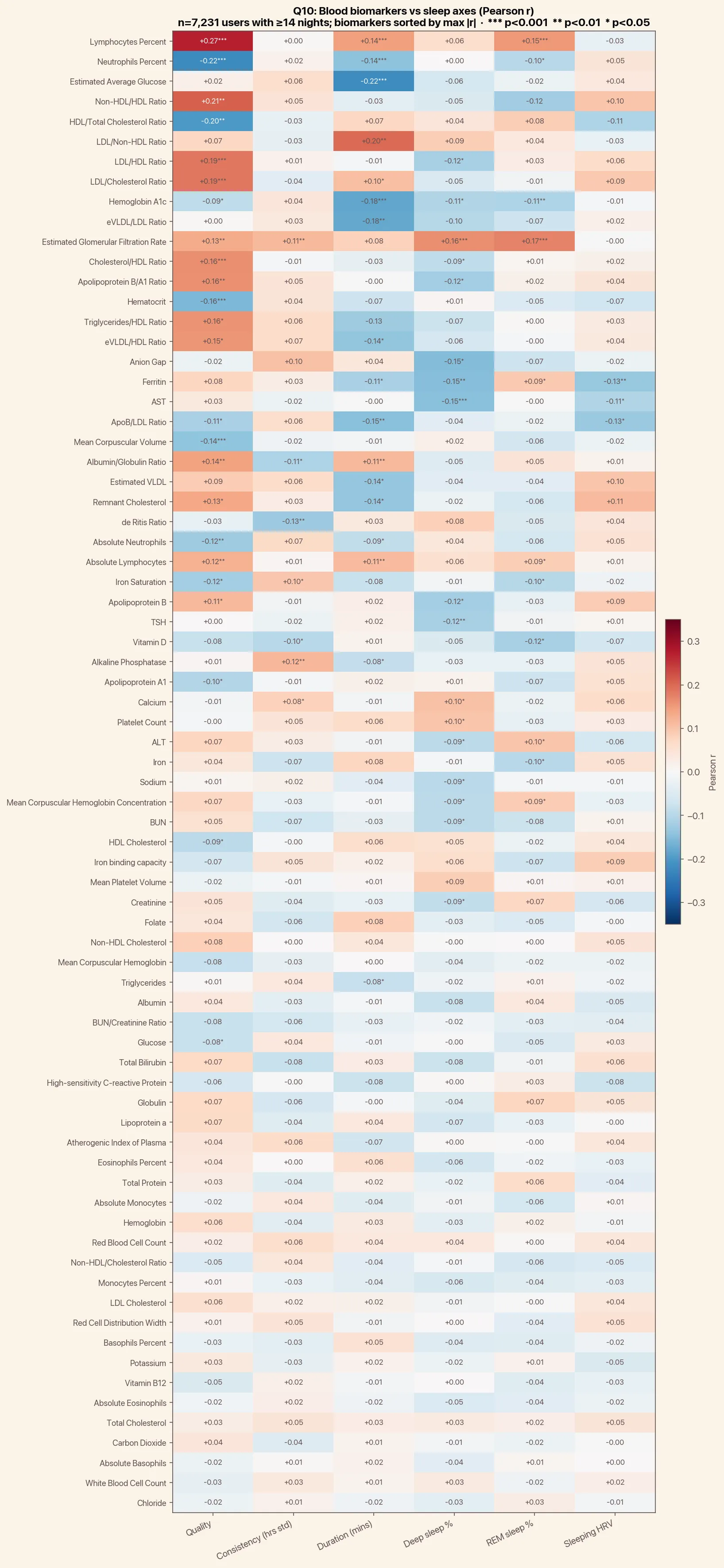
The strongest single correlation in the entire matrix is between sleep quality and lymphocyte percentage (r=+0.272, n=527, p<10⁻¹⁰). The mirror image is neutrophil percentage, which falls as quality rises (r=-0.223, p<10⁻⁷).
Lymphocytes up, neutrophils down: that’s a textbook sign of lower acute inflammation and a better-rested adaptive immune system. The neutrophil-to-lymphocyte ratio is a well-validated stress marker, and we see it moving in the expected direction with better sleep. The same shift shows up against duration (r=+0.144 for lymphocytes, r=-0.144 for neutrophils) and REM sleep %, which makes the immune-balance story the most internally consistent finding in the dataset.
Sleep duration and blood sugar
The next clearest story is metabolic. Sleep duration correlates negatively with hemoglobin A1c (r=-0.181, n=583, p<10⁻⁵) and with estimated average glucose (r=-0.220, n=233, p<0.001). More short nights, higher glucose levels weeks later. A1c moves in the expected direction against every sleep dimension we tested (duration, REM %, deep %, and quality all negative), which makes this finding very robust to how you slice “good sleep.”
This matches the published literature well. The classic Spiegel et al. studies in The Lancet showed reduced insulin sensitivity after just four nights of sleep restriction, and large UK Biobank analyses link short sleep to type 2 diabetes risk. Our cross-sectional data is consistent with both.
Deep sleep and organ function
Deep sleep, the slowest, most restorative stage, lines up with three organ-function and inflammation markers. Kidney filtration (eGFR) rises with both deep sleep % (r=+0.162) and REM sleep % (r=+0.173). The liver enzyme AST falls with deep sleep % (r=-0.147), and so does ferritin (r=-0.150), which doubles as an iron-storage and inflammation marker.
These are smaller correlations than the immune and glucose findings, but the directions are clean: more time in restorative stages, better kidney filtration, lower liver-stress and inflammation markers. We can’t tell from cross-sectional data whether deep sleep improves these markers or whether healthier organs allow more deep sleep, but both are biologically plausible.
What this analysis can and can’t tell you
These are observational correlations, not causal estimates, and they’re unadjusted for age, sex, BMI, and other behavioral confounders. People who sleep well also tend to do other things well. If you want a cleaner dose-response curve, we analyzed noise vs sleep in an attempt to isolate one variable.
What the matrix does show is which biomarkers are worth watching as you change sleep behavior. If you’re working on sleep duration, expect glucose and A1c to move first. If you’re working on sleep quality more broadly, watch your CBC, especially the neutrophil and lymphocyte percentages. The lipid panel is unlikely to budge much from sleep alone, so don’t expect your cholesterol numbers to swing because you slept an extra hour.
Get your free 30-day heart health guide
Evidence-based steps to optimize your heart health.
